|
Unit 8
Neonatal Reflexes and testing reflexes
TOPICS COVERED
Neonatal reflexes Disorders
UNIT CONTENT
Those primitive primate reflexes
Neonatal reflexes
Doll’s Eye reflex: When a baby’s head is manually turned, the eyes will stay fixed, instead of moving with the head. This reflex will disappear at about 1 month.
Galant reflex: While stroking a baby's back to one side, the spine and trunk will arch toward that side.
Moro Reflex: Also called the startle reflex. If the baby’s head is not supported the arms will thrust outward and then seem to embrace themselves as the fingers curl. This reflex disappears at about 2 months of age.
Sucking reflex: This reflex occurs when something is placed in the baby's mouth. It ensures that the baby will nurse on a breast or bottle. This reflex is gradually replaced by voluntary sucking around 2 months of age.
Babinski reflex: When the baby’s foot is stroked from heel toward the toes the big toe should lift up, while the others fan out. Absence of reflex may suggest immaturity of the spinal cord. The Babinski reflex may be present up to 1 year. After that the stroking should elicit a downward curling of the toes.
Babkin reflex: When both of baby's palms are pressed, her eyes will close, mouth will open and her head will turn to one side. The Babkin reflex will disappear around 3-4 months.
Rooting reflex: When the baby’s cheek is stroked, it will turn towards the source of the stimulation, usually looking for food. This reflex can be self-induced as the baby fails its arms. This reflex is generally disappears by about 4 months.
Stepping reflex: If a baby’s feet are placed on a flat surface while the upper body is supported, the baby will “walk by placing one foot in front of the other. This isn't really walking and will disappear by about 4 months of age.
Asymmetrical Tonic Neck reflex: Also called the fencing reflex, because of the position the baby assumes. When the baby turns its head to one side the arms and legs will extend on that side. The opposite arm and leg will flex – thus the “fencing” position. This reflex will disappear about the 4 month.
Symmetrical Tonic Neck reflex: When a baby’s head is flexed forward both arms flex and the legs extend. Conversely, when the head is extended backwards, the arms extend and the legs flex. This reflex is will disappear about the 4 month.
Asymmetrical tonic neck reflex Asymmetrical tonic neck reflex and you
Perez reflex: If a baby’s spine is firmly stroked from tail to head, the baby will cry out and head will rise. The Perez reflex should disappear by 4-6 months
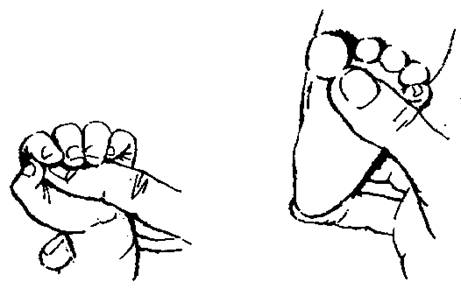
Palmar Grasp reflex: When the palm is touched the fingers will curl around and cling to a finger or object. This is the reflex that allows the baby to “hold hands until it disappears at about 6 months.
Swimming reflex: If babies are placed in water, they will move their arms and legs while holding their breath. This reflex will disappear around the 6 month
Withdrawal reflex: A pin prick to the sole of baby's foot will result in knee and foot flexion.
1st Required QUIZ
Please take in : www.uh.edu/webct You will have 8 minutes to complete the Required Quiz Testing Reflexes
The Knee Jerk Intact reflexes require · intact sensory afferent nerves (coming to the spinal cord) · intact synapse within the spinal cord · intact efferent motor nerves coming from the spinal column · Adequately functioning muscle. Reflexes can also be modified by conditions higher in the cord than the relevant synapse including the brain itself. The purpose of testing reflexes is to check the integrity of the system as a whole. An absent reflex indicates a problem somewhere in the reflex arc but it does not tell you where. Individual elements can often be tested separately by checking muscle power and sensation. General principles of reflex testing· Explain to the patient what you are going to do. ("I’m just going to tap you on the arms with this - show patellar hammer") · Help them to relax ("Just let me hold your legs") · In the case of tendon reflexes stretch the tendon as much as you can before you tap it with the patellar hammer. · Apply stimulus · Observe response · Interpret response The purpose of this session is to give you expertise in testing the main tendon reflexes. The Knee Jerk
1. What it is.
2. What it tests.
3. The stimulus
4. How to elicit it
5. Grade and interpret the response
6. Confirm the finding 7. Test the other side 8. What can go wrong · You find no reflex because the patient is not relaxed. · You find no reflex because the striking the patient’s knee is painful. They have some other problem there. · You poked at the tendon rather than striking it sharply. The tendon has to be stretched fairly quickly to elicit the reflex · You have missed the tendon. The Ankle Jerk
1. What it is.
2. What it tests.
3. The stimulus 4. How to elicit it
5. Grade and interpret the response This is the same as for the knee jerk 6. Confirm the finding · Repeat the observation 7. What can go wrong · You find no reflex because the patient is not relaxed. · The reflex may appear to be absent in women because they find the position undignified even when properly covered. Use the alternative method described below. · You find no reflex because the striking the patient’s ankle is painful. They have some other problem there. · You poked at the tendon rather than striking it sharply. The tendon has to be stretched fairly quickly to elicit the reflex. · You have missed the tendon. 12. An alternative method. A quicker and easier method, that is just as effective, does not involve externally rotating the hip.
The Biceps Jerk
1. What it is.
2. What it tests.
3. The stimulus 4. How to elicit it
5. Grade and interpret the response This is the same as for the knee jerk 6. Confirm the finding Repeat the observation 7. Test the other side. This requires some manual dexterity. Check how the hammer is held picture · 8. What can go wrong o You find no reflex because the patient is not relaxed. o You find no reflex because the striking the patient’s arm is painful. They have some other problem there. o You poked at the tendon rather than striking it sharply. The tendon has to be stretched fairly quickly to elicit the reflex. o You did not stretch the tendon enough to start with.
The Triceps Jerk
1. What it is.
2. What it tests.
3. The stimulus 4. How to elicit it
5. Grade and interpret the response This is the same as for the knee jerk 6. Confirm the finding Repeat the observation 7. Test the other side. 8. What can go wrong · You find no reflex because the patient is not relaxed. · You find no reflex because the striking the patient’s arm is painful. They have some other problem there. · You poked at the tendon rather than striking it sharply. The tendon has to be stretched fairly quickly to elicit the reflex. · You did not stretch the tendon enough to start with. · You hit the muscle and not the tendon. Muscle contraction under these circumstances is a direct response and not dependent on an intact reflex arc.
The Supinator Jerk
1.What it is.
2. What it tests.
3. The stimulus 4. How to elicit it
5. Grade and interpret the response This is the same as for the knee jerk 6. Confirm the finding Repeat the observation 7. Test the other side. 8. What can go wrong · The commonest problem is failure to identify the supinator tendon properly. · You find no reflex because the patient is not relaxed. · You find no reflex because the striking the patient’s arm is painful. They have some other problem there. · You poked at the tendon rather than striking it sharply. The tendon has to be stretched fairly quickly to elicit the reflex. · You did not stretch the tendon enough to start with. · You hit the muscle and not the tendon. Muscle contraction under these circumstances is a direct response and not dependent on an intact reflex arc.
The Plantar Reflex
1.What it is.
2. What it tests.
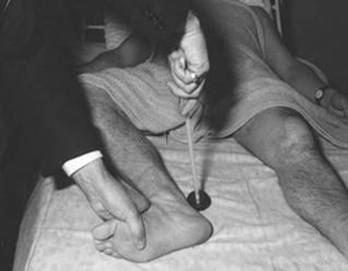
3. The stimulus 4. How to elicit it
5. Grade and interpret the response Under normal circumstances the toe will go down. In patients with upper motorneurone lesions it will go up and the toes will tend to fan out. This is called ‘an extensor plantar response’ or a ‘positive Babinski sign’. Sometimes the toe will go up and down – it is the initial movement that counts. 6. Confirm the finding Only do this if you are really not sure what happened. Eliciting the plantar response is unpleasant. 7. Test the other side. 8. What can go wrong · The toe did not move at all. The patient may have sensory loss over the sole of the foot or your stimulus was not strong enough. · The patient jerks their foot away as soon as you start to scratch it. You did not warn them what you were going to do or the stimulus was too strong. For some people quite small stimulus is enough, just a scratch with the back of your thumbnail will do. 2nd Required QUIZ
Please take in
:
www.uh.edu/webct You will have 13 minutes to complete the Required Quiz |
|||||||||||||||||||||||||||||||||||||