Spinal Cord Injury
Topics Covered
About SCI
Secondary Damage
Applied Regeneration
Current Interventions
UNIT CONTENT
Introductory video - This takes some time to download, be patient.
WHAT IS A SPINAL
CORD INJURY (SCI)?
Spinal Cord Injury (SCI) is
damage to the spinal cord that results in a loss of function such as mobility or
feeling. Frequent causes of damage are trauma (car accident, gunshot, falls,
etc.) or disease (polio, spina bifida, Friedreich's Ataxia, etc.). The spinal
cord does not have to be severed in order for a loss of functioning to occur. In
fact, in most people with SCI, the spinal cord is intact, but the damage to it
results in loss of functioning. SCI is very different from back injuries such as
ruptured disks, spinal stenosis or pinched nerves.
A person can "break their back or neck" yet not sustain a spinal cord injury if
only the bones around the spinal cord (the vertebrae) are damaged, but the
spinal cord is not affected. In these situations, the individual may not
experience paralysis after the bones are stabilized (Spinal Cord Injury resource
center, 2006).
WHAT ARE THE EFFECTS OF A
SCI?
The effects of SCI depend on the
type of injury and the level of the injury. SCI can be divided into two types
of injury - complete and incomplete. A complete injury means that there is no
function below the level of the injury; no sensation and no voluntary movement.
Both sides of the body are equally affected. An incomplete injury means that
there is some functioning below the primary level of the injury. A person with
an incomplete injury may be able to move one limb more than another, may be able
to feel parts of the body that cannot be moved, or may have more functioning on
one side of the body than the other. With the advances in acute treatment of
SCI, incomplete injuries are becoming more common.
The level of injury is very helpful in predicting what parts of the body
might be affected by paralysis and loss of function. Remember that in incomplete
injuries there will be some variation in these prognoses.
Cervical (neck) injuries usually result in quadriplegia.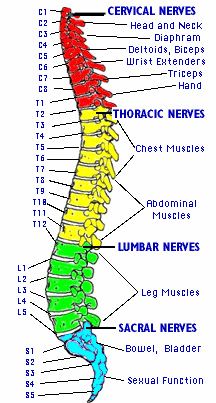 Injuries above the C-4 level may require a ventilator for the person to breathe.
C-5 injuries often result in shoulder and biceps control, but no control at the
wrist or hand. C-6 injuries generally yield wrist control, but no hand function.
Individuals with C-7 and T-1 injuries can straighten their arms but still may
have dexterity problems with the hand and fingers. Injuries at the thoracic
level and below result in paraplegia, with the hands not affected. At T-1 to T-8
there is most often control of the hands, but poor trunk control as the result
of lack of abdominal muscle control. Lower T-injuries (T-9 to T-12) allow good
truck control and good abdominal muscle control. Sitting balance is very good.
Lumbar and Sacral injuries yield decreasing control of the hip flexors and legs.
Injuries above the C-4 level may require a ventilator for the person to breathe.
C-5 injuries often result in shoulder and biceps control, but no control at the
wrist or hand. C-6 injuries generally yield wrist control, but no hand function.
Individuals with C-7 and T-1 injuries can straighten their arms but still may
have dexterity problems with the hand and fingers. Injuries at the thoracic
level and below result in paraplegia, with the hands not affected. At T-1 to T-8
there is most often control of the hands, but poor trunk control as the result
of lack of abdominal muscle control. Lower T-injuries (T-9 to T-12) allow good
truck control and good abdominal muscle control. Sitting balance is very good.
Lumbar and Sacral injuries yield decreasing control of the hip flexors and legs.
Besides a loss of sensation or motor functioning, individuals with SCI also
experience other changes. For example, they may experience dysfunction of the
bowel and bladder,. Sexual functioning in men may affect their fertility
resulting in a low sperm count, while women's fertility is generally not
affected. Very high injuries (C-1, C-2) can result in a loss of many involuntary
functions including the ability to breathe, necessitating breathing aids such as
mechanical ventilators or diaphragmatic pacemakers. Other effects of SCI may
include low blood pressure, inability to regulate blood pressure effectively,
reduced control of body temperature, inability to sweat below the level of
injury, and chronic pain (Spinal cord injury resource center, 2006).
HOW MANY PEOPLE HAVE A SCI?
WHO ARE THEY?
Approximately 450,000 people
live with SCI in the US. There are about 10,000 new SCI's every year; the
majority of them (82%) involve males between the ages of 16-30. These injuries
result from motor vehicle accidents (36%), violence (28.9%), or falls
(21.2%).Quadriplegia is slightly more common than paraplegia (Spinal cord injury
resource center, 2006).
Complications following a SCI
Secondary complications can develop following a spinal cord injury and
necessary steps should be taken to prevent these complications. Following
is a list of possible complications, please be sure and read all the material on
each of the websites to get a clear understanding of the complications that can
arise following a SCI.
Pressure ulcers,
Bladder
Autonomic
dysreflexia
Osteoporosis,
Spasticity I
Spasticity II
Spasticity Video
Spinal Cord Lesion: Effects and Perspectives of
Treatment - article
WHERE DAMAGE OCCURS
MATTERS
Researchers studying spinal cords obtained from autopsy
have identified several different types of spinal cord
injuries. The most common types of spinal cord injuries
found in one large study were contusions (bruising of
the spinal cord) and compression injuries (caused by
pressure on the spinal cord). Other types of injury
included lacerations, caused by a bullet or other
object, and central cord syndrome.
In contusion injuries, a cavity, or hole, often forms in
the center of the spinal cord. Myelinated axons
typically survive in a ring along the inside edge of the
cord. Some axons may survive in the center cavity, but
they usually lose their myelin covering. This
demyelination greatly slows the speed of nerve
transmission. Slowing of nerve impulses can be measured
by a diagnostic technique called transcranial magnetic
stimulation (TMS).
Another example of a spinal cord injury is central cord
syndrome, which affects the cervical (neck) region of
the cord and results from focused damage to a group of
nerve fibers called the corticospinal tract. The
corticospinal tract controls movement by carrying
signals between the brain and the spinal cord. Patients
with central cord syndrome typically have relatively
mild impairment, and they often spontaneously recover
many of their abilities. Patients usually recover
substantially by 6 weeks after injury, despite continued
loss of axons and myelin. Delays in motor responses
persist, but permanent impairment is usually confined to
the hands.
Complete severing of the spinal cord is rare in humans,
but even axons that survive the initial injury often
lose their ability to function. Secondary damage, which
continues for hours, can cause loss of myelin,
degeneration of axons, and nerve cell death. Patients
with their spinal cords completely severed often show
abnormal reflexes that emerge more than 8 months after
injury. These reflexes, such as twitching of muscles in
the arm and hand in response to sensory stimulation of
the legs and feet, may result from "sprouting" of new
branches from sensory fibers just below the lesion. They
may also result from activation of nerve pathways that
are normally suppressed. Other abnormal responses, such
as sweating in response to movement of a hair, may be
due to sprouting of nerves in the autonomic nervous
system. The autonomic nervous system is the part of the
PNS that controls involuntary body functions such as
sweating and heart rate.
Article pertaining
to damage and recovery
SECONDARY
DAMAGE
1. Immune System Reactions